
Online decision tool created by Kaiser Permanente researchers helps emergency room doctors identify low-risk patients with a pulmonary embolism
*This story was updated May 16, 2022. It was first published Nov. 12, 2018.
A decision support tool implemented in Kaiser Permanente Northern California emergency departments in 2016 has continued to help physicians safely discharge patients with an acute pulmonary embolism to their homes without harmful effects, a new Kaiser Permanente study shows. An acute pulmonary embolism is a blood clot that blocks blood flow to the lungs.
The study was published May 16 in JAMA Network Open. Researchers in Kaiser Permanente’s Clinical Research on Emergency Services and Treatments (CREST) Network developed and then initially evaluated the implementation of an online support tool, called RISTRA (RIsk STRAtification), in 2016. Their research showing the tool could be successfully implemented was published in 2018 in Annals of Internal Medicine.
“Our online tool helps emergency room doctors to quickly and easily identify which patients with pulmonary embolism can be safely treated at home, thus avoiding costly and inconvenient hospitalization,” said lead author David R. Vinson, MD, an adjunct investigator with the Kaiser Permanente Division of Research and an emergency department physician with The Permanente Medical Group (TPMG).
RISTRA incorporates evidence-based risk stratification recommendations for pulmonary embolism. It can be completed automatically from the patient’s electronic health record. Its use is physician-driven and not linked to a pop-up alert or prompt.
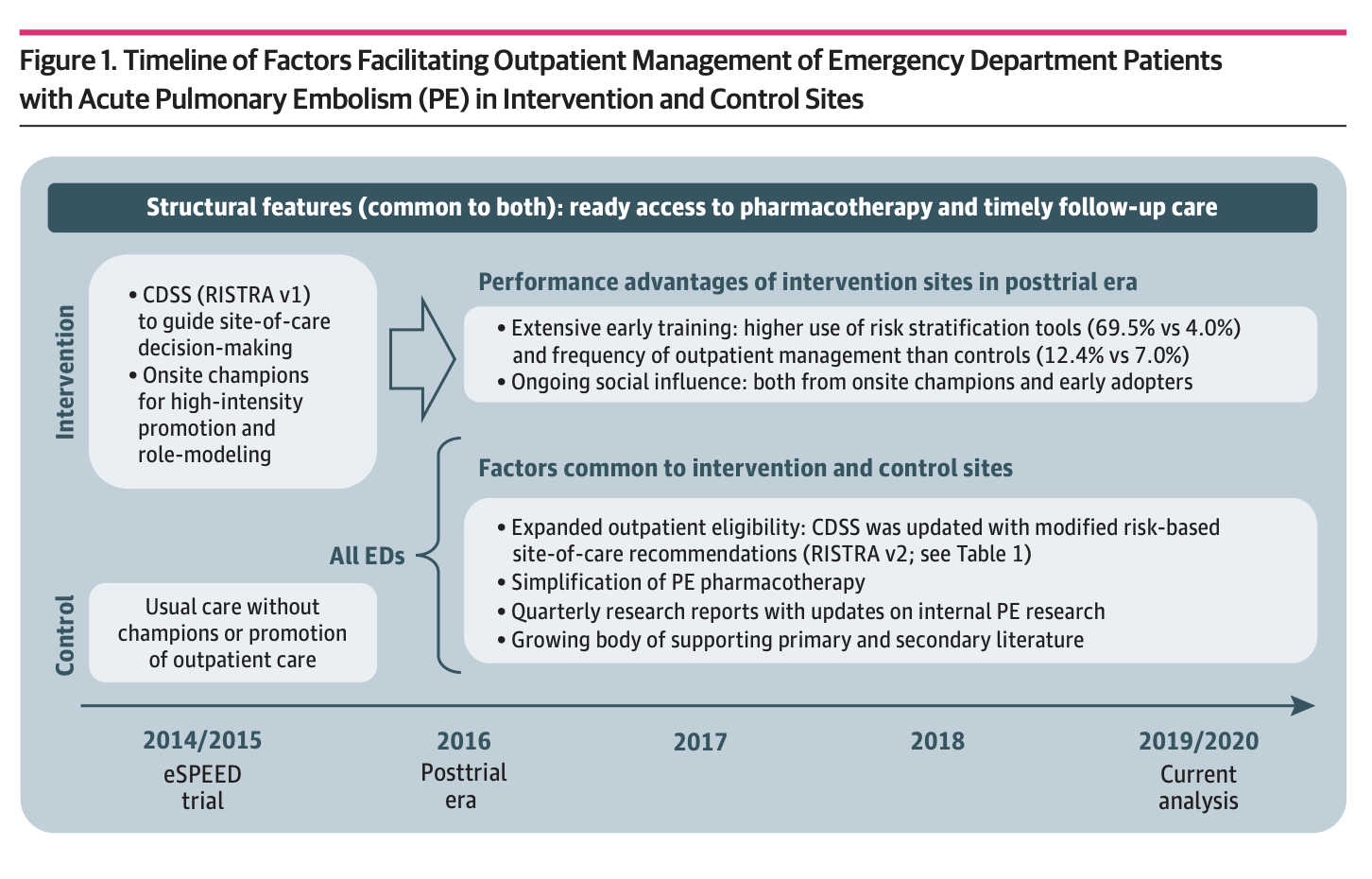
The new study evaluated the tool’s use in 1,039 patients seen between January 2019 to February 2020 at all 21 Kaiser Permanente Northern California emergency departments. All emergency departments began using the tool in 2016. The new study compared use at the 10 intervention emergency departments with use at the 11 control sites used in the original implementation study.
During the original study, the intervention sites had a physician “champion” promote use of the risk tool. The new study found that outpatient management of patients increased significantly in the 11 emergency departments that served as control sites. But the 10 emergency departments that had had champions continued to have more low-risk patients who were discharged home: 46% of the low-risk patients seen at the 10 intervention hospitals were discharged compared with 34% of the low-risk patients at the former control sites.
Was that a heart attack, or not?
The symptoms of pulmonary embolism can overlap with those of heart attacks, making it more difficult to diagnose. “The most common symptoms of pulmonary embolism are shortness of breath, and chest pain,” Vinson said. “Because of the clot, the lungs have to work extra hard.”
However, tests done in the emergency department, including electrocardiograms and blood tests, can definitively rule out heart attacks, Vinson said. The diagnosis of pulmonary embolism, on the other hand, is usually made with a CT (computed tomography) scan.
 “Then the doctor must decide whether a patient with pulmonary embolism is a good candidate for home care, can be sent to a short-term observation unit, or is best-served by hospitalization.”
“Then the doctor must decide whether a patient with pulmonary embolism is a good candidate for home care, can be sent to a short-term observation unit, or is best-served by hospitalization.”
Onsite “champions”
The original study was conducted in 21 emergency departments in Kaiser Permanente Northern California from January 2014 to April 2015, with 10 intervention and 11 control sites. The RISTRA decision support tool for pulmonary embolism was available to doctors in the 10 intervention sites.
At the intervention sites, doctors were educated about the tool; got positive feedback by email after using the tool; and received a small incentive for each of their first three uses of RISTRA. In addition, a physician “champion” promoted use of the tool at intervention sites.
“We weren’t directing our physicians’ site-of-care decisions,” said study co-author Dustin W. Ballard, MD, MBE, an adjunct investigator with the Division of Research and an emergency department physician with TPMG. “We were informing them. We wanted the physicians in conversation with their patients to decide what was the best site of care.”
The original study enrolled 881 patients with pulmonary embolism at intervention sites and 822 patients at control sites. In emergency departments with the intervention:
- 70 percent of doctors with patients with acute pulmonary embolism consulted the RISTRA tool before making their decision on whether to admit the patient.
- The rate of home discharge for patients with acute pulmonary embolism increased 60 percent, from 17 percent before the intervention to 28 percent afterward. In this study we defined home discharge more broadly: it included discharge either from the emergency department or after a short-term stay (less than 24 hours) in outpatient observation.
- The intervention sites did not have any increase in people with acute pulmonary embolism returning to the emergency department within 5 days or adverse outcomes within 30 days.
$1 billion in possible costs savings
Vinson and co-authors estimate that for every 100 emergency department patients with acute pulmonary embolism, the intervention averted 11 unnecessary hospitalizations.

“With an average hospital stay of three days, costing about $2,300 per day, that would add up to about $80,000 in cost savings per 100 patients,” Vinson said.
In an editorial that accompanied the original study, Paul D. Stein, MD, and Mary J. Hughes, DO, of Michigan State University College of Osteopathic Medicine, wrote that despite some challenges in implementing the tool, the benefits of broad implementation in emergency departments would include a significant reduction in health care costs.
“The investigators are to be congratulated for showing the effectiveness of this computer tool that, when intensively promoted, enabled physicians to knowledgeably select a larger proportion of patients for home treatment,” they wrote.
Stein and Hughes pointed out that if all eligible patients with pulmonary embolism seen in U.S. emergency departments were treated at home rather than in the hospital, health care costs would decrease by $1 billion per year.
“The clinical decision support tool for pulmonary embolism benefits all players,” Vinson said. “Physicians receive evidence-based guidance on how to provide optimal care, patients receive the intensity of care that best matches their needs, and the health care system at large is enabled to better manage its resources.”
The study was funded by the Garfield Memorial National Research Fund, The Permanente Medical Group Delivery Science and Physician Researcher programs, Kaiser Permanente Northern California Community Benefit Program, and the Kaiser Permanente Innovation Fund for Technology.
Co-authors include Dustin G. Mark, MD, Uli Chettipally, MD, MPH, Jie Huang, PhD, Adina S. Rauchwerger, MPH, Mary E. Reed, Dr.PH, James S. Lin, MD, Mamata V. Kene MD, MPH, Dana R. Sax, MD, MPH, Ian D. McLachlan, MD, MPH, and Andrew R. Elms, MD, of the CREST Network; David H. Wang, MD, Scripps Health, Tamara S. Pleshakov, DO, Kaiser Permanente Los Angeles Medical Center, Cyrus K. Yamin, MD, Kaiser Permanente Oakland Medical Center, Hilary R. Iskin, BA, University of Michigan Medical School, and Ridhima Vemula, BA, University of Cincinnati College of Medicine; and Donald M. Yealy, MD, University of Pittsburgh School of Medicine.




This Post Has 0 Comments