
Kaiser Permanente study finds not all such patients need to go through the emergency department
Some people who get blood clots in their lungs may be able to skip a visit to the emergency department and be managed safely by their primary care physicians, a new Kaiser Permanente analysis suggests. The study was published January 12 in the Journal of General Internal Medicine.
While most patients at risk of pulmonary embolism and with symptoms — chest pain and trouble breathing — go straight to the hospital for assessment, some go first to their primary care doctor. This study by Kaiser Permanente’s CREST Network assessed how the latter group of patients fare by examining 646 patients who were diagnosed with acute pulmonary embolism in primary care at Kaiser Permanente Northern California between 2013 and 2019.
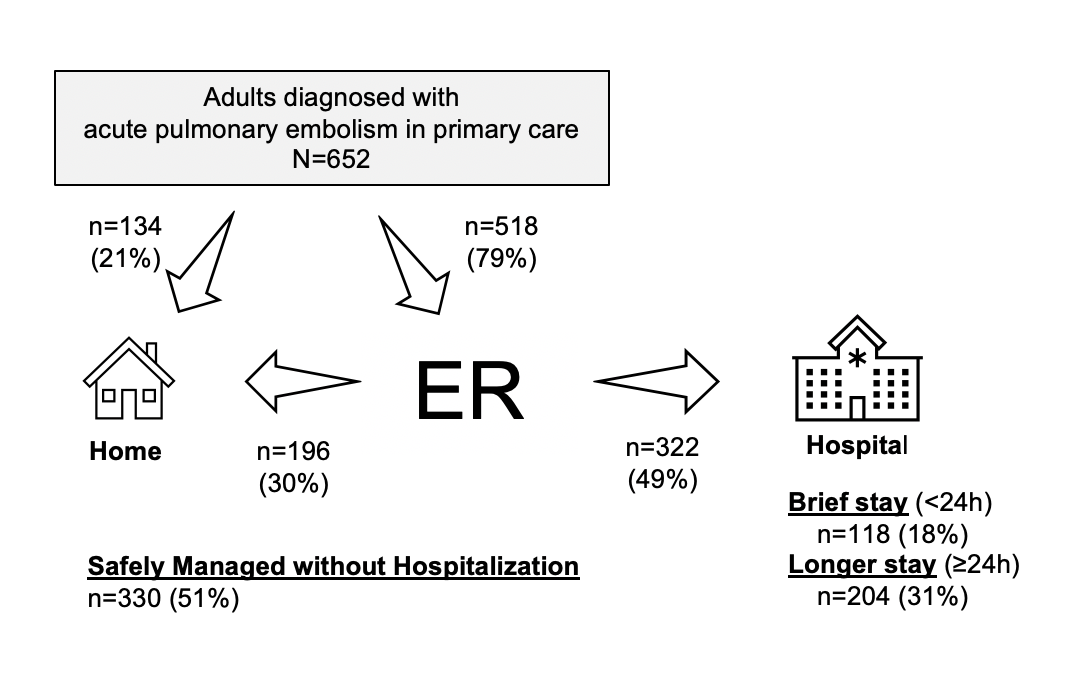
Most of the patients (about 80%) were diagnosed by their primary care clinician and then sent to an emergency department or hospital, but the rest were diagnosed and sent home with a treatment plan. Adverse events were rare.
The results suggest pulmonary emboli of mild or moderate risk may be handled by primary care clinicians safely, said lead author David Vinson, MD, adjunct investigator with the Kaiser Permanente Division of Research and an emergency medicine specialist with The Permanente Medical Group.
“The safety outcomes we found were very reassuring and show that comprehensive management of pulmonary embolism in primary care is a feasible option,” Vinson said. “It was a sign that the doctors know how to select patients appropriately for this type of care.”
Pulmonary embolism is a blood clot in a lung artery. A pulmonary embolism typically starts as a blood clot in the leg (deep vein thrombosis) that breaks off and travels to the lungs. A pulmonary embolism can cause permanent damage to the lung, low blood oxygen levels, or damage to the heart; it can be life threatening if the clot is large or there are many clots.
Risk for developing pulmonary embolism is increased for people after major surgery, as well as those who are immobilized for long periods, such as those in a leg cast, or in bed with an illness such as flu or COVID-19. Symptoms include chest pain and shortness of breath. Diagnosis may involve an EKG, chest X-ray, and a blood test, with ultimate diagnosis often made using a CT scan of the lungs.
 “We knew that patients were getting a diagnosis from their primary care doctor because as an ER physician, I would see patients come in from the clinic with their diagnosis in hand,” Vinson said. “But the characteristics of this primary care population and their management – and their outcomes – had never been described before in the medical literature.”
“We knew that patients were getting a diagnosis from their primary care doctor because as an ER physician, I would see patients come in from the clinic with their diagnosis in hand,” Vinson said. “But the characteristics of this primary care population and their management – and their outcomes – had never been described before in the medical literature.”
Of 652 encounters with 646 patients diagnosed with pulmonary embolism in primary care, 518 (79.5%) were referred by their doctors to the emergency department or hospital and 134 (20.5%) were sent home with a treatment plan. Only one patient who was sent home had an adverse event within 30 days, a recurrent pulmonary embolism.
Of the total, 8 patients experienced a serious adverse event within 30 days of diagnosis: 4 new or worsening clots, 1 major bleed and 3 deaths. The 3 deaths were all patients with known metastatic cancer who were hospitalized and enrolled in hospice.
The study also found that patients diagnosed with pulmonary embolism in primary care were a lower-risk population than those diagnosed in the emergency department. That may be because patients did not feel their symptoms were serious enough to go to the ER, or because the primary care clinician determined the patient was a good candidate for an outpatient evaluation.

“Primary care physicians maintain important, long-term relationships with patients, and use their clinical judgment to assess patients with potential pulmonary embolism and triage them to appropriate next steps,” said Sameer Awsare, MD, associate executive director for The Permanente Medical Group. “Research like this is essential to building evidence-based clinical pathways to assist clinicians in providing safe, effective care and a good care experience for patients.”
Embolism management
A small minority of pulmonary embolism patients diagnosed in the clinic needed intensive care management in the hospital, Vinson said. Most can get blood thinners (anticoagulants) and be monitored in the hospital or recover at home. The question is whether primary care physicians feel comfortable managing patients without sending them to the ER or hospital, he said.
“With this condition, there is not yet a recommended clinical pathway developed for primary care physicians to follow,” Vinson said. “But we found that doctors were selecting patients appropriately for comprehensive clinic-based care because patients rarely ran into trouble. There could be an opportunity here to expand the practice by providing primary care physicians with some clinical decision support on how to make the diagnosis and which patients would be low-risk and safe for comprehensive clinic-based care.”
One caveat noted by the study authors: the results reflect coordination of care and patient support available within Kaiser Permanente’s integrated care model. Kaiser Permanente’s primary care clinicians can order CT scans and patients on anticoagulants receive education and close follow-up by an anticoagulation management service, which may not be the case outside an integrated system
The study was funded by a Kaiser Permanente Community Health grant and The Permanente Medical Group Delivery Science and Applied Research Program.
Study co-authors were Mary Reed, DrPH, Jie Huang, PhD, Judy Shan, BS, Adina Rauchwerger, MPH, of the Division of Research; Dustin Mark, MD, Erik R. Hofmann, MD, Suresh Rangarajan, MD, MSc, and Karen L. Wallace, MD, of The Permanente Medical Group; and Elizabeth J. Johnson, MD, and Dayna J. Isaacs, MD, MPH, of the University of California, Davis.
# # #
About the Kaiser Permanente Division of Research
The Kaiser Permanente Division of Research conducts, publishes and disseminates epidemiologic and health services research to improve the health and medical care of Kaiser Permanente members and society at large. It seeks to understand the determinants of illness and well-being, and to improve the quality and cost-effectiveness of health care. Currently, DOR’s 600-plus staff is working on more than 450 epidemiological and health services research projects. For more information, visit divisionofresearch.kaiserpermanente.org or follow us @KPDOR.




This Post Has 0 Comments